

the boring committee that should be at the center of the vaccine debate
Meet the real heroes: The Advisory Committee on Immunization Practices.

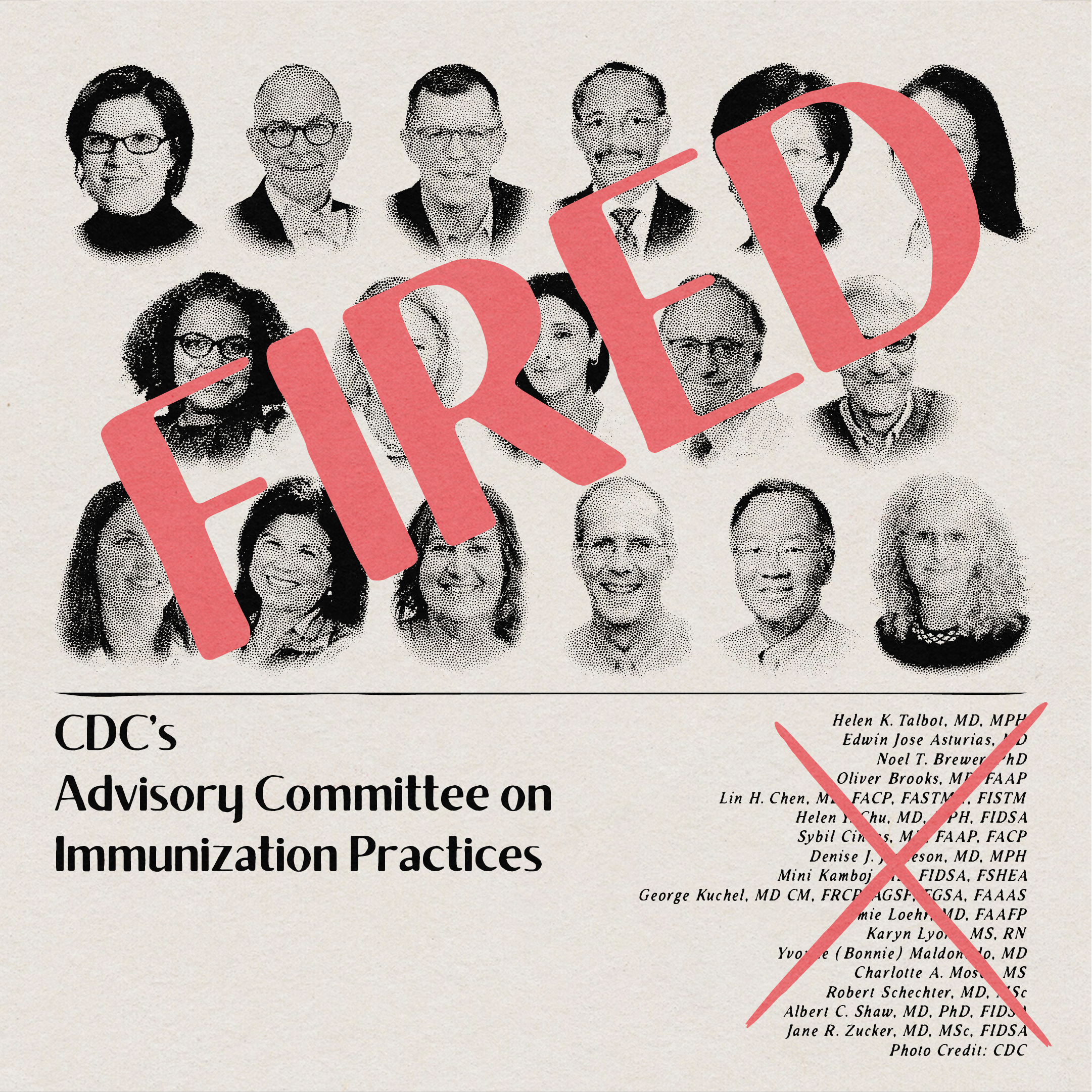
Updated June 10: Since this post was made, RFK Jr. fired everyone on ACIP, the committee discussed in this post.
Last week, the FDA Commissioner, Marty Makary, and his advisor, Vinay Prasad, issued a statement piece via The New England Journal of Medicine titled “An Evidence-Based Approach to COVID-19 Vaccination.” The headlines quickly followed:
FDA may limit future Covid-19 shots to older people and those at risk of severe infection. -CNN
F.D.A Poised to Restrict Access to Covid Vaccines. -New York Times
Fall Covid vaccine rollout for healthy kids, adults is likely not going to happen -NBC News
This news caught me by surprise.
Then this week, @SecKennedy (HHS) posted a video to X announcing that “he couldn’t be more pleased to announce” that COVID vaccines would not be recommended for healthy children AND pregnant women. They aren’t even consistent in their policies?
Who is making policy here? HHS? FDA? NIH? CDC? Is this coordinated with last week’s message? Is this even from the CDC?
There are definitely problems with their policies, but the greater concern is that it’s not their policy to make in the first place.
It’s the job of the Advisory Committee on Immunization Practices (ACIP). According to their website (which is part of the CDC), “ACIP comprises medical and public health experts who develop recommendations on the use of vaccines in the civilian population of the United States.” ACIP is exactly the sort of entity we want making those decisions!
It’s transparent—the public can offer comments, and their sessions are live-streamed and recorded. They even publish every potential conflict of interest back to 2000. Here is their manual on how to make evidence-based recommendations! ACIP doesn’t just make decisions about COVID either. Last summer, there were 10 separate vaccines on the agenda.
The wildest part is that ACIP is scheduled to meet on June 25-27 to discuss this very issue. Instead, two dudes with no experience in making vaccine policy just issued a memo out of turn. And then three dudes made a video about the same thing but differently, making things even less clear.
But what do you expect from political appointees with access to a job title, soapbox, and an agenda, am I right?
What to know about the statement piece.
Last week’s statement piece rationalizes the change to vaccinating only high-risk populations because 1) “it aligns them more with the policies of peer countries” and 2) it will give them time to “demand robust, gold-standard data on persons at low risk.”
I’ll concede Makary and Prasad their first point—that different countries do things differently—to focus on the second. They imply we are missing robust, gold-standard data on COVID vaccines in low-risk people. COVID vaccines were recommended because of strong data, not despite it.
Despite their best efforts, I remain utterly unconvinced this is true—and you know me, I read the whole thing top to bottom looking for evidence. Not only does their report disintegrate under the gentlest scrutiny, but their credibility declined the further down the rabbit hole I fell.
This memo is a pair of vaccine skeptics in a trench coat. My thoughts, in no particular order, after reading the entire memo:
Makary and Prasad cite their own research to support the new policy. The other citations are straightforward, such as links to previous CDC policies. I certainly understand a researcher citing their earlier work, but it has “I’m smart enough to do this because I wrote a big boy paper” energy.
There is no mention of long COVID in this memo at all. Evidence-based public policy regarding COVID cannot be taken seriously without considering long COVID.
Makary and Prasad hilariously accuse other experts of “arguing that the American people are not sophisticated enough to understand age- and risk-based recommendations.” The same Americans who get their babies’ MMR vaccinations at 12-15 months and 4-6 years? The same ones who get tetanus shots every 10 years, or if they get a puncture wound? You cannot be serious.
They use low COVID vaccination rates to support their stance on reducing vaccine availability. That’s a rookie critical thinking error. Take seatbelts. It would be like saying, “seatbelts work, but because some people don’t like them, we’ve decided to stop recommending them for everyone.”
Makary and Prasad insist they want to restore public trust in vaccines. They provide no evidence that vaccine are anything less than safe except vague conspiracy theory sounding bullshit.
They say, “We simply don’t know whether a healthy 52-year-old woman with a normal BMI who has had Covid-19 three times and has received six previous doses of a Covid-19 vaccine will benefit from the seventh dose.” That’s not a problem with the science. That’s just what happens when a novel virus drops from the sky, we make a vaccine in a year, and get about five years down the road.
Not surprisingly, a 2022 paper co-authored by Makary concluded that requiring booster shots in young people would cause more injury than benefit—a mind-boggling claim. Dr. Robert Morris of the University of Washington published a critique of that study:
“They made mistake after mistake and every time it either minimized the vaccine's benefits or exaggerated the risks.” This paper really fed the whole notion that the vaccine is worse than the disease.”
This memo does exactly that.
What to know about the video posted to X.
Not even a week later, on Tuesday, Dr. Marty Makary was flanked by Secretary Kennedy and the head of the NIH, Dr. Jay Bhattacharya, on a video release X. It also addresses COVID vaccines, but contradicts last week’s statement. It’s just one minute long—no Q&A and no detail.
Just a big change to the immunization schedule: healthy pregnant women won’t get COVID vaccines.

No one from the CDC was present. There was no mention of this news on the CDC website or the CDC’s X account. In fact, there is no confirmed CDC director at all right now.
The internet did an admirable job of immediately listing all the reasons why Kennedy’s recommendations to exclude healthy pregnant people from the COVID list are potentially shortsighted.
Babies have comparable COVID hospitalization rates to the elderly.
Pregnant people are at a higher risk of COVID complications, including hospitalizations and death.
Babies who are born to unvaccinated people won’t even have acquired immunity from being in utero, putting them at greater risk. (Babies hospitalized for COVID were much more likely to have a mother who had not been vaccinated for COVID.)
No mention of long COVID, despite the vaccine showing modest protection for long COVID specifically in children.
No clarity on whether unvaccinated children should get at least one COVID shot.
Concern over whether insurance companies will cover the vaccine costs for people who want them.
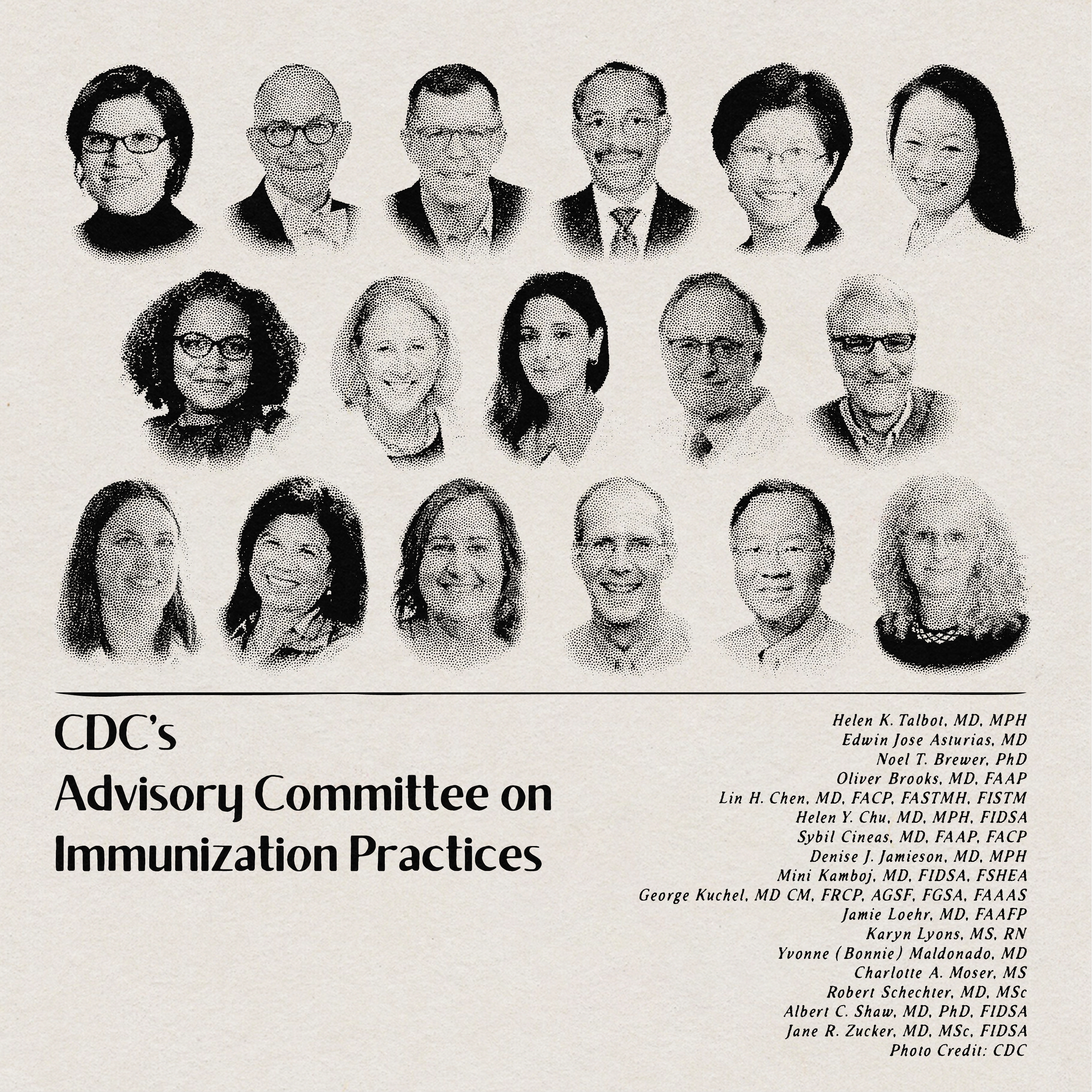
Who makes up ACIP?
The American people deserve to have these issues debated in the correct venue—ACIP. By the way, if you would like to see the individuals who are qualified to do that work and part of ACIP, here the 17 current voting members:
The committee includes experts on:
Epidemiology of COVID, influenza, and RSV
Prevention of infection and morbidity in adults
Advancing research on vaccine-preventable diseases and improving healthcare delivery in underserved regions
Behavioral and social drivers of vaccine uptake
Disparities in vaccine coverage rates
Large-scale community surveillance studies
Teaching about and promoting vaccination in the clinical setting
Emerging infections and vaccines in pregnancy
Improving vaccination in those with immunocompromising conditions
Geriatrics and gerontology
Pediatric infectious diseases
Developing educational materials about vaccines
Immune system function in older adults
Vaccine-preventable diseases outbreak control and emergency preparedness
They will be joined by six representatives from federal agencies and 30 non-voting members who provide expertise from their liaison organizations, comprising doctors, nurses, and other medical specialists.
As for now, ACIP is still scheduled to meet, and they will open the floor to public comments on June 9. I sure hope there is a confirmed, qualified CDC director to review their recommendations.
Here is what an excerpt of last year’s recommendations looked like. This is way more complex than the average person can understand. It’s highly specialized work that requires an understanding of medicine, research, economics, public policy, and epidemiology.

These vaccines are being vetted by people who are being extremely transparent and issuing public reports with citations. It’s right there in front of us!
Do we think Kennedy, Makary, Prasad, or Bhattacharya understand what monovalent or “generally lower VE” mean?
The Department of Health and Human Dis-Services
Last night, it was announced that the Department of Health and Human Services (HHS) had canceled a Biden-era contract with Moderna for an H5N1 vaccine that’s currently showing promising results in early trials. Despite Moderna’s success in creating a vaccine with a “rapid, potent, and durable immune response,” the HHS pulled the plug.
I expect other countries might be willing to pick up the bill and enjoy the fruits of that labor if the H5N1 pandemic ever comes to pass—an unlikely but possible event.
HHS Communications Director Andrew Nixon said in a statement: “After a rigorous review, we concluded that continued investment in Moderna's H5N1 mRNA vaccine was not scientifically or ethically justifiable.”
"This is not simply about efficacy — it's about safety, integrity, and trust. The reality is that mRNA technology remains under-tested, and we are not going to spend taxpayer dollars repeating the mistakes of the last administration, which concealed legitimate safety concerns from the public," Nixon said.
He added that "the move signals a shift in federal vaccine funding priorities toward platforms with better-established safety profiles and transparent data practices. HHS remains committed to advancing pandemic preparedness through technologies that are evidence-based, ethically grounded, and publicly accountable." The official did not provide any additional details.” - NPR, Rob Stein
Did he say, “better-established safety profiles and transparent data practices”? No offense to him, but has he actually read how these trials were conducted? Was he present when children were being injected with experimental vaccines, and did he see the safeguards in place?
Because I was: I actually enrolled my children in Pfizer’s mRNA COVID vaccine trials.
Get ready to nerd out about mRNA vaccines and take a peek into a real COVID-era mRNA vaccine trial.
In light of all this news, it seems like a good time to tell you about that. As you can imagine, it was no small decision to allow my children to participate in a trial, especially one with “new” technology. I’ll take you through my research on mRNA vaccines, explain how they work, and tell you about what the trial was actually like.
Plus, I’m ready to nerd out and create some diagrams. I’ve got several graphics ready to go and am thrilled to share them with you. In college, I taught a hands-on class about protein folding to a class of octogenarians at NC State’s Lifelong Learning Center in the mid-2000s and received a 5/5 rating. If they loved that, I promise I can make learning about mRNA fun!
Vaccine skepticism isn’t new. Now that we are seeing it at the public policy level, it feels harder to combat misinformation with “trust me, I’m a scientist.” Regular people want to understand for themselves how these things work so they can interpret the mixed messaging.
Talk soon!
P.S. Angela Alsobrooks (D-MD) patiently crafted RFK Jr. an entirely new asshole on the floor of the Senate using the power of his own contradictory statements. My favorite quote: “We can roll back the tape, you absolutely did say that.” If you would also enjoy that, here’s the link.
Boring, yes, but vital